Головна сторінка Випадкова сторінка
КАТЕГОРІЇ:
АвтомобіліБіологіяБудівництвоВідпочинок і туризмГеографіяДім і садЕкологіяЕкономікаЕлектронікаІноземні мовиІнформатикаІншеІсторіяКультураЛітератураМатематикаМедицинаМеталлургіяМеханікаОсвітаОхорона праціПедагогікаПолітикаПравоПсихологіяРелігіяСоціологіяСпортФізикаФілософіяФінансиХімія
Адміністративний договір
Дата добавления: 2015-09-15; просмотров: 1097
|
|
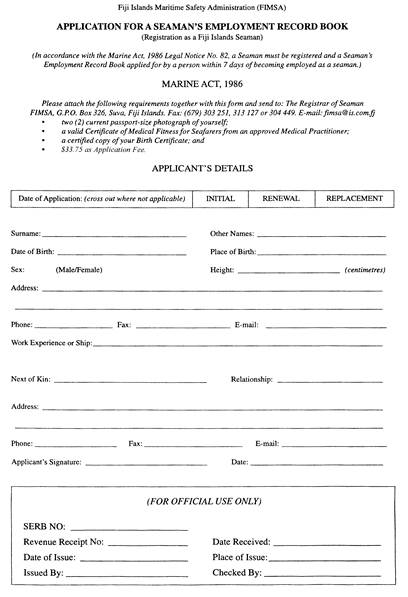
| Date of application: Дата подачи заявления: | |||
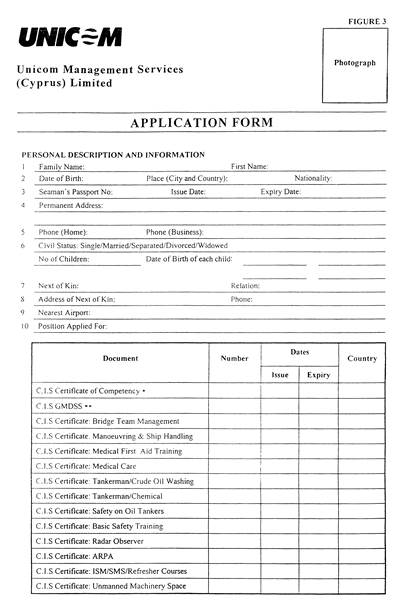
| Last Name: Фамилия: | Other Names: Другие имена: | ||
| Date of Birth: Дата Рождения: | Place of Birth: Место Рождения: | ||
| Sex: (Male/ Female) Пол: (Мужской/ женский) | Height: Рост: | ||
| Address: Адрес: | |||
| Phone: Телефон: | Fax: Факс: | E-mail: Электронный адрес: | |
| Work Experience or Ship: Опыт Работы или Судно: | |||
| Next of Kin: Ближайшие Родственники: | Relationship: Степень родства: | ||
| Address: Адрес: | |||
| Phone: Телефон: | Fax: Факс: | E-mail: Электронный адрес: | |
| Applicant’s Signature: Подпись Заявителя: | Date: Дата: | ||
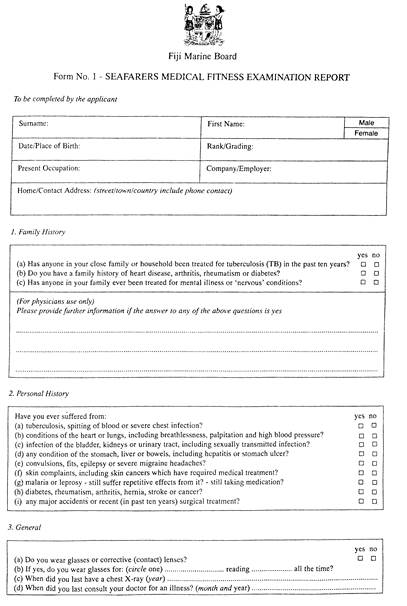
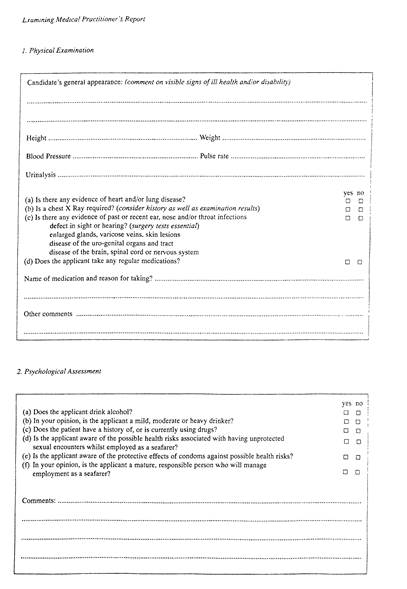
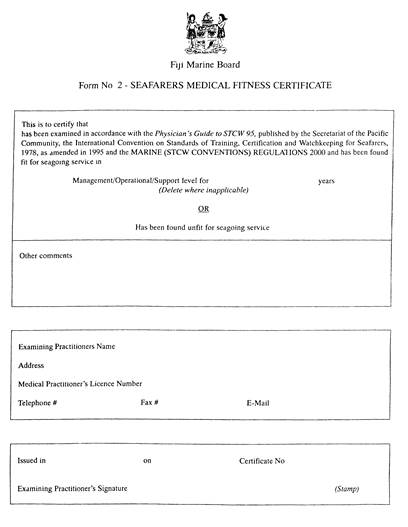
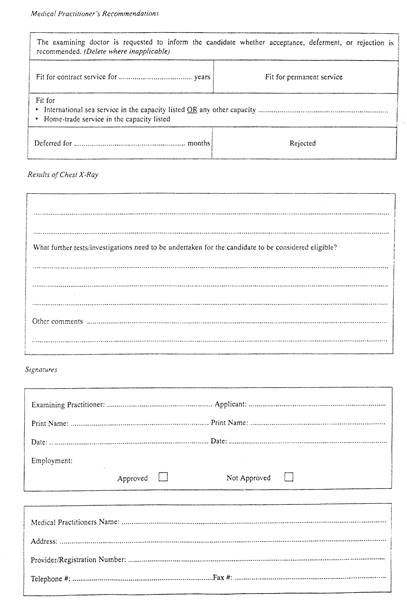
EXAMINATION AND CERTIFICATION OF SEAFARERS: COMPENDIUM
ANNEX 2
| The Republic of lIberia ministry of finance bureau of maritime affairs | PHYSICAL EXAMINATION REPORT/CERTIFICATE | ||||||||||||
| LAST NAME OF APPLICANT | FIRST NAME | MIDDLE INITIAL | |||||||||||
 DATE OF BIRTH
MONTH DAY YEAR DATE OF BIRTH
MONTH DAY YEAR
| PLACE OF BIRTH CITY COUNTRY | ||||||||||||
| EXAMINATION FOR DUTY AS: MASTER * MATE * ENGINEER * RADIO OFF * SEAMAN * | MAILING ADDRESS OF APPLICANT | ||||||||||||
| MEDICAL EXAMINATION (SEE REVERSE SIDE FOR MEDICAL REQUIREMENTS) STATE DETAILS ON REVERSE SIDE | |||||||||||||
| HEIGHT | WEIGHT | BLOOD PRESSURE | PULSE | RESPIRATION | GENERAL APPEARANCE | ||||||||
| VISION: RIGHT EYE LEFT EYE | HEARING: RT EAR_______________________LEFT EAR___________________________ | ||||||||||||
| WITHOUT GLASSES | |||||||||||||
| WITH GLASSES | |||||||||||||
| COLOR TEST TYPE: BOOK * LANTERN * | Check if color test is normal | " YELLOW________RED_____GREEN________BLUE______ | |||||||||||
| HEAD AND NECK ______________________________________________ | HEART (CARDIOVASCULAR) ___________________________________________________________ | ||||||||||||
| LUNGS _______________________________________ ______________________________________________ | |||||||||||||
| SPEECH (RADIO OFFICER): Is speech unimpaired for normal voice communication?_____________________________________________________________________________________________ | |||||||||||||
| EXTREMITIES: UPPER ___________________________________________ LOWER_______________________________________________________________ | |||||||||||||
| Is applicant suffering from any disease likely to be aggravated by or to render him unfit for service at sea or likely to endanger the health of other persons onboard? | |||||||||||||
| _________________________________________________ ________________________________ SIGNATURE OF APPLICANT DATE This signature be attired in the presence of the examining Physician THIS IS TO CERTIFY THAT A PHYSICAL EXAMINATION WAS GIVEN TO:__________________________________________________________________________ (Name of Applicant) | |||||||||||||
| (HE) (SHE) IS FOUND TO BE (FIT) (NOT FIT) FOR DUTY AS A | |||||||||||||
| (MASTER, MATE, ENGINEER, RADIO OFFICER OR SEAMAN) NAME AND DEGREE OF PHYSICIAN__________________________________________________________________________________________________________ (PLEASE PRINT) ADDRESS _______________________________________________________________________________________________________________________________ NAME OF PHYSICIAN’S LICENSING AUTHORITY_______________________________________________________________________________________________ DATE OF ISSUE OF PHYSICIAN’S LICENSE____________________________________________________________________________________________________ SIGNATURE OF PHYSICIAN_________________________________________________________________________________________________________________ | |||||||||||||
This certificate is issued by authority of Liberian Maritime Regulation 10.325(2) and in compliance with the requirements
of the Medical Examination (Seafarers) Convention 1946 (ILO No/ 73)
ANNEX 2
| <== предыдущая лекция | | | следующая лекция ==> |
| Проблема адміністративного договору у законодавстві, теорії, на практиці | | | АДМІНІСТРАТИВНИЙ ДОГОВІР ЯК ВАЖЛИВА ФОРМА ДІЯЛЬНОСТІ ПУБЛІЧНОЇ АДМІНІСТРАЦІЇ - Міхровська М.С. |